View this page in: English | Nederlands
Testosterone is a steroid hormone from the androgen group. Testosterone is secreted in the testes of male bodied people and the ovaries of female bodied people. It is the principal male sex hormone and the “original” anabolic steroid. In both males and females, it plays key roles in health and well-being. Examples include enhanced libido, energy, immune function, and protection against osteoporosis.
Taking T
You need to have your blood monitored regularly by your doctor when on T. It needs to be monitored for cholesterol, hormone levels, liver function, hematocrit (percentage of red blood cells in the blood), and a few other things (please add to this!). Your blood must also be taken shortly before you start T, so that your doctor has a baseline of information to compare everything to. Generally you have bloodwork done after 6 months on T, after another 6 months (when you’re 1 year on T), and every year after that. Your doctor may want you to have it done more frequently if you have specific health concerns.
Comparison of methods
See http://community.livejournal.com/ftm/1288249.html for a comparison of injections vs. patches vs. gel, pros and cons, etc.
Injections
Injections are by far the most common and the least expensive, although expensive is unlikely to be a consideration for those transitioning on the NHS in the UK. Different forms of injectable testosterone are prescribed in different countries, with the brand Sustanon (a mix of fast- and slow-acting esters) being most common in the United Kingdom.
Many, many people who are on injections have a fear of needles; some have a serious phobia. Many of these same people discover that they are able to self-inject after they’ve been on T for a while. There are a number of strategies for dealing with fear of needles; it need not stop you from going on injectable T. If you suffer from such a phobia and wish to use injectable testosterone, consult your doctor for resources in overcoming this. This is particularly important if you suffer from vasovagal syncope (also known as vasovagal reflex reaction and malignant vasovagal syndrome), a potentially life-threatening condition associated with some forms of needle phobia. In addition to your doctor, the Needle Phobia Information Project at http://www.needlephobia.info/ and other online resources can provide help with these problems.
See http://community.livejournal.com/ftm/2532795.html for a guide to self-injecting in the arse, which does not require you to be a contortionist and is entirely feasible even if you’re a bigger guy.
If you’re in the US, see http://imed.com/shop/sections/index.cfm/s/636979 for cheap syringes and needles available without a prescription. Also in the US, if you get your T through http://stroheckersrx.com/, they can send you syringes and needles with your T.
If you inject, be aware that the smaller the gauge of your needle, the larger its number. An 18 gauge needle is very large. A 30 gauge needle is very small. The smallest (and therefore least painful) gauge that anyone who reports to T-Vox uses to inject is 27. You can draw up with as large a needle as you like, and the larger the needle, the faster the drawing-up time. A 25 may take a few minutes; a 20 takes perhaps 15 seconds.
As for the length of the needle you use to inject, a 1.5-inch needle is entirely unnecessary. Most folks will want a 1-inch needle; some may prefer a half-inch needle. It is generally understood that injecting into subcutaneous fat rather than muscle has no detrimental effect; not all doctors are ready to trust that, though. (It is common practice in South Africa and other parts of the world, and is slowly gaining popularity in the US.) If you self-inject, it is your decision and no one else’s what size needle you use. As long as your testosterone levels are in the ideal range, you’re fine.
Stabbing into the vial to get your T significantly dulls the needle, which makes it more painful. You should be exchanging it for a new one before you inject. Other problems with injectable testosterone can include an allergy to the oil in which the testosterone is suspended, and a fluctuation in mood due to the intervals between injections.
The patch
The patch causes skin irritation in everyone. This is the point of the patch. It has to irritate the skin in order to allow the T to pass through and into the bloodstream. If you’re allergic to the adhesive, the irritation will be all the worse. Even without an allergy to the adhesive, the irritation may be bad enough that you have raised red welts on your skin (which will itch like a motherfucker), and may even resemble burns. Your endo or GP may have to prescribe steroid cream to apply to them (Elocon 0.1% cream is one used in the US); for those who wish to avoid such creams, a topical application of natural remedies such as aloe vera or lavender oil may alleviate the irritation to some extent. You cannot put a new patch on the irritated skin until it has completely healed; this may mean that you have to wear them on your thighs sometimes because you’re completely out of upper-arm and shoulder space (note that the AndroPatch brand commonly prescribed in the UK recommends several areas of the body for application). However, some trans men find that the convenience, lack of needles and steady mood of the patches outweighs the irritation, particularly at the start of their medical transition.
Other forms
Other forms of testosterone include gel, cream, depo injection (in the United Kingdom, the brand “Nebido” is used) and sublingual and buccal tablets. Oral testosterone is less commonly prescribed, due to the effect of methyltestosterone on the liver; however, testosterone undecanoate is considered safer and sometimes prescribed outside the US. (Please add to this!)
Sources of testosterone
Like other steroid hormones, testosterone is derived from cholesterol. The largest amounts of testosterone are produced by the testes in men, but it is also synthesised in smaller quantities in women by the theca cells of the ovaries, by the placenta, as well as by the zona reticulosa of the adrenal cortex in both sexes.
In the testes, testosterone is produced by the Leydig cells. Due to the dual function of the male gonad, testosterone directly influences spermatogenesis. Like most hormones, testosterone is supplied to target tissues in the blood where much of it is transported bound to a specific plasma protein, sex hormone binding globulin (SHBG).
Mechanism of effects
The effects of testosterone in humans and other vertebrates occur by way of two main mechanisms: by activation of the androgen receptor (directly or as DHT), and by conversion to estradiol and activation of certain oestrogen receptors.
Free testosterone (T) is transported into the cytoplasm of target tissue cells, where it can bind to the androgen receptor, or can be reduced to 5α-dihydrotestosterone (DHT) by the cytoplasmic enzyme 5α-reductase. DHT binds to the same androgen receptor even more strongly than T, so that its androgenic potency is about 2.5 times that of T. The T-receptor or DHT-receptor complex undergoes a structural change that allows it to move into the cell nucleus and bind directly to specific nucleotide sequences of the chromosomal DNA. The areas of binding are called hormone response elements (HREs), and influence transcriptional activity of certain genes, producing the androgen effects.
Androgen receptors occur in many different vertebrate body system tissues, and both males and females respond similarly to similar levels. Greatly differing amounts of testosterone prenatally, at puberty, and throughout life account for a large share of biological differences between males and females.
The bones and the brain are two important tissues in humans where the primary effect of testosterone is by way of aromatisation to estradiol. In the bones, estradiol accelerates maturation of cartilage into bone, leading to closure of the epiphyses and conclusion of growth. In the central nervous system, testosterone is aromatised to estradiol. Estradiol rather than testosterone serves as the most important feedback signal to the hypothalamus (especially affecting LH secretion). In many mammals, prenatal or perinatal “masculinisation” of the sexually dimorphic areas of the brain by estradiol derived from testosterone programs later male sexual behaviour.
Effects of testosterone on humans
In general, androgens promote protein synthesis and growth of those tissues with androgen receptors. Testosterone effects can be classified as virilising and anabolic effects, although the distinction is somewhat artificial, as many of the effects can be considered both.
Anabolic effects include growth of muscle mass and strength, increased bone density and strength, and stimulation of height growth and bone maturation.
Virilizing effects include maturation of the sex organs, particularly the penis and the formation of the scrotum in foetuses, and after birth (usually at puberty) a deepening of the voice, growth of the beard and torso hair.
Many of these fall into the category of male secondary sex characteristics. Increased testosterone causes deepening of the voice in both sexes at puberty. To take advantage of its virilising effects, testosterone is often administered to trans men (female-to-male transsexual and transgender people) as part of the hormone replacement therapy, with a “target level” of the normal male testosterone level. Likewise, transsexual women are prescribed drugs (anti-androgens) to decrease the level of testosterone in the body and allow for the effects of oestrogen to develop. Testosterone is also often used by bodybuilders to enhance muscle build.
Testosterone effects can also be classified by the age of usual occurrence. For postnatal effects in both males and females, these are mostly dependent on the levels and duration of circulating free testosterone.
Prenatal androgen effects
Most of the prenatal androgen effects occur between 7 and 12 weeks of gestation.
- Genital virilisation (midline fusion, phallic urethra, scrotal thinning and rugation, phallic enlargement)
- Development of prostate and seminal vesicles
Early infancy androgen effects
Early infancy androgen effects are the least understood. In the first weeks of life for male infants, testosterone levels rise. The levels remain in a pubertal range for a few months, but usually reach the barely detectable levels of childhood by 4-6 months of age. The function of this rise in humans is unknown. It has been speculated that “brain masculinisation” is occurring since no significant changes have been identified in other parts of the body.
Early postnatal effects
Early postnatal effects are the first visible effects of rising androgen levels in childhood, and occur in both males and females in puberty.
- Adult-type body odour
- Increased oiliness of skin and hair, acne
- Pubarche (appearance of pubic hair)
- Axillary hair
- Growth spurt, accelerated bone maturation
- Fine upper lip and sideburn hair
Advanced postnatal effects
Advanced postnatal effects begin to occur when androgen has been higher than normal adult female levels for months or years. In males these are normal late pubertal effects; however, they only occur in female-bodied people after prolonged periods of excessive levels of free testosterone in the blood.
- Phallic enlargement, including clitoromegaly. Whether it’s a clitoris or a penis, it’s the same organ, and testosterone will make it grow, although the penis—which averages at 5-6 inches when erect—will always be larger than the clitoris, which might get to be 3 inches erect.
- Increased libido and erection frequency
- Pubic hair extends to thighs and up toward umbilicus (navel)
- Facial hair (sideburns, beard, mustache)
- Chest hair, periareolar (around the nipples) hair, perianal (on your butt) hair
- Increased muscle strength and mass
- Deepening of voice
- Growth of spermatogenic tissue in testes (male fertility—sperm is being produced)
- Growth of jaw and remodelling of facial bone contours
- Completion of bone maturation and termination of growth. This occurs indirectly via estradiol metabolites and hence more gradually in men than women.
Adult testosterone effects
Adult testosterone effects are important in adult males, and may decline as testosterone levels decline in the later decades of adult life.
- Maintenance of muscle mass and strength
- Maintenance of bone density and strength
- Libido and erection frequency
- Mental and physical energy
Michael Exton, Tillmann Krüger et al. examined the effect of a 3-week period of sexual abstinence on the neuroendocrine response to masturbation-induced orgasm. [1]
“The procedure was conducted for each participant twice, both before and after a 3-week period of sexual abstinence. Plasma was subsequently analysed for concentrations of adrenaline, noradrenaline, cortisol, prolactin, luteinizing hormone and testosterone concentrations. Orgasm increased blood pressure, heart rate, plasma catecholamines and prolactin. These effects were observed both before and after sexual abstinence. In contrast, although plasma testosterone was unaltered by orgasm, higher testosterone concentrations were observed following the period of abstinence. These data demonstrate that acute abstinence does not change the neuroendocrine response to orgasm but does produce elevated levels of testosterone in males.”
Therapeutic use of testosterone
Testosterone was first isolated from a bull in 1935. There have been many pharmaceutical forms over the years. Forms of testosterone for human administration currently available in North America include testosterone cypionate and enanthate in oil for injection, methyltestosterone tablets for oral ingestion, and skin patches and a gel preparation for transdermal absorption. A buccal oral preparation is also available. In the pipeline are a “roll on” delivery method and a nasal spray. Both are under development.
The original and primary use of testosterone is for the treatment of males who have little or no natural testosterone. The benefits can include the relief of depression and anxiety, and tiredness. It is not an immediate effect and the benefits can take several months to become apparent. Regular contact with the relevant specialist is highly recommended.
However, over the years, as with every hormone, testosterone or other anabolic steroids has also been given for many other conditions and purposes besides replacement, with variable success but higher rates of side effects or problems. Examples include infertility, lack of libido or erectile dysfunction, osteoporosis, penile enlargement, height growth, bone marrow stimulation and reversal of anaemia, and even appetite stimulation. By the late 1940s testosterone was being touted as an anti-ageing wonder drug (e.g., see Paul de Kruif’s The Male Hormone) in exactly the same way that growth hormone is being described today.
Anabolic steroids have also been taken to enhance muscle development, strength, or endurance. After a series of scandals and publicity in the 1980s (such as Ben Johnson’s improved performance at the 1988 Summer Olympics), prohibitions of anabolic steroid use were renewed or strengthened by many sports organisations, and it was made a “controlled substance” by the United States Congress.
Ongoing investigations are also exploring the use of testosterone as a male contraceptive. Exogenous administration of testosterone suppresses pituitary production of gonadotropins by negative feedback inhibition. This also suppresses testicular testosterone production and sperm production decreases significantly as a result. Testosterone as a contraceptive is still in the trial stage, and is not currently available for use.
The “testosterone deficiency” of ageing and the andropause controversy
The latest development in testosterone use appears to be a reprise of the anti-ageing claims. A number of physicians, supported by pharmaceutical manufacturers, are popularising the concept that the testosterone decline of ageing (which they term the “andropause”) is unnecessary and can be treated. Many endocrinologists suspect that this issue will play out like post-menopausal oestrogen replacement: use will increase until large trials demonstrate (1) the benefits are much less dramatic or assured than when treating deficiency, and (2) a higher incidence of side effects like prostate cancer will occur associated with this type of use.
Synthesis
Testosterone is synthesised from pregnenolone, the precursor of all steroid hormones and a derivative of cholesterol.

The synthesis of all androgens starts with the hydroxylation of C-17 of progesterone, to yield 17α-hydroxyprogesterone. The side chain is cleaved to form androstenedione.
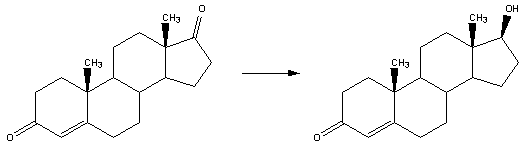
The keto group on C-17 is reduced to an alcohol to yield testosterone. Testosterone is a potential precursor of estradiol.
External links
- NIST Standard Reference Database
- Testosterone information from Dimensions at the Castro-Mission Health Centre in San Francisco, California, US.
- More testosterone information from FORGE
- Still more testosterone information from the US National Library of Medicine
- Medical Therapy and Health Maintenance for Transgender Men: A Guide For Health Care Providers – written by a physician who is also FTM and has treated FTMs.
Latest comments